Review of Hip Musculature and Impact of Dynamic Back Design
Michelle L. Lange, OTR/L, ABDA, ATP/SMS
Review of Hip Musculature and Impact of Dynamic Back Design
Michelle L. Lange, OTR/L, ABDA, ATP/SMS
It’s been a long time since I took an anatomy class and unfortunately, like most students, I did not yet have any clinical context. I wanted to take a closer look at this, particularly in relation to how a client interacts with a Dynamic Back.
Donald A. Neumann, PT, PhD, FAPTA wrote an in-depth clinical commentary of “Kinesiology of the Hip: A Focus on Muscular Actions” in the Journal of Orthopaedic & Sports Physical Therapy. I ran across this recently and found his commentary very helpful.
 Muscles of the Hip
Muscles of the Hip
A whopping 21 muscles cross the hip – and I’m absolutely certain I can’t name them all. These muscles provide movement in 3 planes and provide stability between the femur and acetabulum (the hip joint). This movement is complex. Movement can occur at just the femur while the pelvis is stationary or at the pelvis while the femur is stationary, trunk muscles typically activate simultaneously, and certain muscles provide compression force at the hip. Muscle torque (strength), moment arm (leverage), and line of force relative to an axis of rotation is all relevant to successful use of a Dynamic Back.
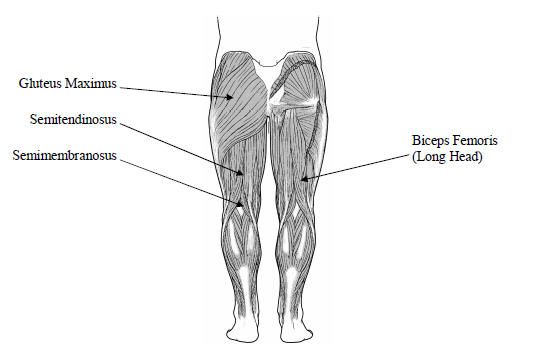
Hip Extensors
A Dynamic Back responds to client forces by opening the seat to back angle. This force is generated by the hip extensors which include the gluteus maximus, posterior head of the adductor magnus, and the hamstrings. “The position of flexion naturally augments the torque potential of the hip extensor muscles” which provides potential force from a seated position (i.e. in a wheelchair seating system). This potential is further increased as the client is able to ‘leverage’ off the seating surface. The hip extensor group produce more torque across the hip than any other muscle group. What are the implications of this? A client seated in a wheelchair can potentially exert strong force into hip extension.
If the trunk is held in a stationary position (such as against a wheelchair back, perhaps with the addition of anterior trunk supports), “contraction of the hip extensors and abdominal muscles … functions as a force-couple to posteriorly tilt the pelvis.” What are the implications of this? Hip extension is likely to lead to posterior pelvic tilt.
The hip extensor group produce more torque across the hip than any other muscle group.
As the hip extensor group can produce strong torque against the hip, often in conjunction with the adductors and internal rotators, the femoral head can rotate away from the acetabulum during extension. In combination with an early lack of weightbearing and ambulation resulting in a shallow hip socket, hip subluxation and dislocation are more likely.
Implications
Most people using a wheelchair do not have typical muscle strength and may also have abnormal muscle tone. However, these muscle groups are typically present, have specific attachments, and work together to effect predictable movements. In clients with abnormal muscle tone, the flexor group is often weaker than the more dominate extensor group. Even if the muscle strength of the extensor group is less than typical, increased tone can result in greater than typical force.
If this force is unrelieved, as with a static seating system, hip extension will continue. The pelvis will be pushed into a posterior tilt and the legs will leverage the pelvis off of the seating surface, elevating the pelvis and further extending the hip joint, resulting in shear forces against the back of the seating system. When hip extension eventually relents, the client is likely to return to the seating surface in a posterior pelvic tilt, resulting in a loss of position with hip extension.
Dynamic Seating
A Dynamic Back will move in response to hip extension, dissipating client force. The dynamic component, such as an elastomer, will absorb and store energy from this force, returning the client to a starting position. If the pivot point matches the natural pivot point of the hip and the seat to back angle does not open excessively, the client will return to a starting position without sliding into a posterior tilt and with minimal shear forces.
The Seating Dynamics Dynamic Rocker Back interface (DRBi) has a raised pivot point that is designed to be close to the natural pivot point of the hip. The back extends about 10 to 15 degrees – enough to diffuse force, but not enough to lead to loss of position or shear forces.
The design of a Dynamic Back must respect the design of the hip musculature and how it works. This will result in a successful intervention for the clients we serve.
Reference: Neumann, D. A. (2010). Kinesiology of the hip: a focus on muscular actions. Journal of Orthopaedic & Sports Physical Therapy, 40(2), 82-94.