What are Primitive Reflexes?
Michelle L. Lange, OTR/L, ABDA, ATP/SMS
Primitive Reflexes, also called obligatory patterns, are commonly seen in people with increased muscle tone. These reflexes are present in infancy and often aid in specific tasks such as nursing. As the child develops, these reflexes are ‘integrated’ and no longer dominate movement patterns. Reflexes may persist due to damage to the brain and/or a lack of typical motor development and movement.
These reflexes are non-progressive, though persistent obligatory patterns can lead to orthopedic changes and loss of range of motion. Functionally, these obligatory patterns may limit volitional control, as motor movement may be dominated by the reflex.
These reflexes are non-progressive, though persistent obligatory patterns can lead to orthopedic changes and loss of range of motion. Functionally, these obligatory patterns may limit volitional control, as motor movement may be dominated by the reflex.
Here are a few common primitive reflexes seen in people with increased muscle tone which can impact positioning and function:
Source: Creative Commons
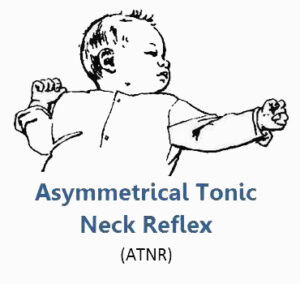
- Asymmetrical Tonic Neck Reflex (ATNR): consistent, one-sided movements of the body when the head is turn where extension occurs on the face side and flexion occurs on the posterior head side.
When this persists, the client may have difficulty visually regarding anything directly in front of them and may become ‘stuck’ on a switch by the side of the head if using this to access assistive technology.
- Symmetrical Tonic Neck Reflex (STNR): is elicited either by neck extension and results in upper extremity extension and lower extremity flexion or by neck flexion resulting in upper extremity flexion and lower extremity extension. This is more commonly seen in children with cerebral palsy (CP) than in typical neonates.
When this is present, the client must be positioned to avoid neck hyperextension or flexion in order to maintain body posture.
- Tonic Labyrinthine Reflex (TLR): tilting the head back in supine causes the back to arch, the lower extremities to extend, and the upper extremities to flex.
When present, the client may not be able to tolerate tilt or recline, as the reflex can be elicited if the head moves posterior of upright.
- Rooting Reflex: this is elicited by a touch on the corner of the person’s mouth and results in the head turning and the mouth opening.
When this persists, a lateral support pad or switch by the cheek may elicit this reflex.
- Stepping Reflex: this is elicited in young babies when upright and the feet touch a solid surface, resulting in stepping movements although the baby cannot yet truly bear weight.
When this persists, the person may have difficulty maintaining contact with a footplate and be observed to frequently lift the foot up off of this surface.
Positioning cannot make primitive reflexes or obligatory patterns go away. However, positioning can be used to inhibit these patterns. It is also important to not place seating components or access methods where a reflex would be elicited. Dynamic Seating can be helpful in absorbing forces which may result during these patterns of movement.
In subsequent blogs in this series, we will address common diagnoses where increased tone is present. We will then address tone management and general seating interventions which can be helpful when working with someone who has increased muscle tone. Finally, we will discuss how Dynamic Seating can be used in conjunction with these strategies to achieve and maintain an optimal position in these circumstances.
For more information, check out our CEU Course on this topic here!
As a recently retired Healthcare Scientist (33 yrs in Rehabilitation Engineering) and now in Swansea University, the subject of Primitive reflexes is something I was taught about early in my career, as a subject it needs promoting and teaching.
Thanks for having the foresight and promoting this subject.
Thank you for your comment, Alan! Primitive reflexes certainly drive posture and movement patterns and need to be addressed in our seating interventions! Michelle Lange